| SSI Assessment Tool 2022.pdf |
| APIC2022 Conference - Breakfast Symposium -- Prevention of SSIs with a 7S Bundle Approach June 14 2022.pdf |
| Spencer M et al Perioperative_Hair_Removal_-_a_Review_of_Best_Practice_-_Journ_Perioper_Nursing_June_2018.pdf |
| Edmiston_et_al-2018- AORN Journal_-_An_Incision_Closure_Bundle_for_Colorectal_Surgery.pdf |
| Spencer M et al Reduction in Colon SSI using a CHG Surgical Irrigant AORN Conference Poster April 2017df |
| 7 S Bundle for Prevention of SSIs. APIC Poster 2014.pdf |
| Spencer M et al.Wound Prevalence Observational Study for the Prevention of Surgical Site Infections AORN April 2016 Poster |
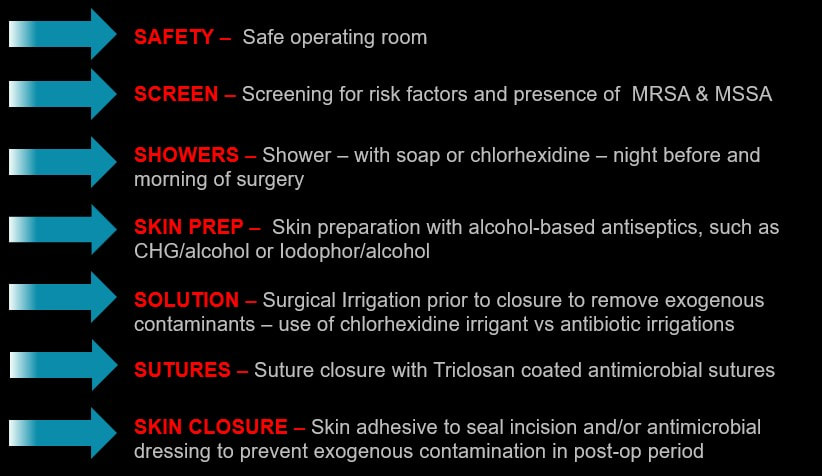
The 7 S Bundle was created by Maureen Spencer, RN, BSN, M.Ed, CIC, FAPIC, Infection Prevention Consultant. This is based on both personal experience and evidenced based practices and it is not intended to suggest product preference or endorsement. Some of the products are unique innovative infection prevention options, while other vendors may not be listed here but are available for your program. Research, guidelines or recommendations are included with each step but are not inclusive of all available information. These are steps to be considered when investigating and evaluating your surgical site infections and prevention program.
1. Safe OR practices: - Evaluate whether you have a safe OR: traffic control, number of staff in the room during surgery, compliance with surgical attire, proper surgical skin scrub, proper skin prep with alcohol based antiseptics, effective sterilization of instruments, monitoring and preventive maintenance of air handling systems, adequate surgical prophylaxis, warming of the patient before and during surgery, hair clipping (no shaving) outside the operating room, use of wound protectors to prevent tissue contamination, careful handling of tissue by surgical staff, disinfection of the environment during room turnovers and terminal cleaning, safe medication handling procedures and safe storage of supplies.
2. Screen – consider screening patients undergoing inpatient surgery for the presence of MRSA and Staph aureus (MSSA) in the nares and screen for pre-op risk factors. Consider rapid technology, such as polymerase chain reaction (PCR) for rapid turnaround time for results (~1 hour).
3. Shower – during the pre-admission testing process or in surgeon’s office – instruct patients who will undergo inpatient surgery to bathe with soap and water, CHG liquid soap or CHG impregnated washcloths (night before and morning of surgery). In addition to showers, the use of universal decolonization with nasal antiseptics in the pre-op holding area before surgery has been shown to reduce SSIs. Nasal antiseptics include 1) alcohol/orange oil/benzalkonium chloride and 2) iodine nasal antiseptics.
4. Skin prep – Use alcohol-based antiseptic skin preps - such as CHG/alcohol, Iodophor/alcohol skin prep, alcohol/functional excipients with citric acid products with long lasting residual effect.
5. Solution – “solution to pollution is dilution” – consider using antiseptic surgical irrigation products, such as 0.05% chlorhexidine irrigant, to remove surgical and environmental contaminants deposited into the surgical field. Discontinue the use of antibiotic irrigations.
6. Sutures – sutures impregnated with a mild antiseptic - Triclosan - as recommended by the SSI guidelines.
7. Skin incisional protection – use of topical skin adhesive to seal the incision post-op or apply over incision a special dressing with antimicrobial agents (e.g. silver, CHG) for duration of hospitalization or longer post-op.
| prolonged_operative_duration_increases_risk_of_ssi_-.pdf |
| parvizi_edmiston_barnes__environment_of_care-_is_it_time_to_reassess_microbial_contamination_of_or_air_as_risk_for_ssi__ajic_sep2017.pdf |
| SSI Fishbone_diagram.ppt |
| antimicrobial-resistant_pathogens_associated_with_hais_sievert_ricks_edwards_et_al.pdf |
